Dr. U.Th.Zierau et PD Dr. W.Lahl
Sealing vein protocol – Our modifications
The super glue VenaSeal has been used by Saphenion for nearly 7 years to treat truncal varicose veins. Of course, after the treatment of 1221 patients and 2290 truncal veins, the therapy scheme is also considered. About modifications to improve the application, to expand the spectrum and – from the perspective of the patient – a more gentle and faster therapeutic success is coming. These results from the large experiences, especially through many long – term follow up are coming from examinations in our patients. There are several ways to modify the course of therapy. The vein glue VenaSeal is also a technique that leaves a lot of room for maneuver and can be adapted individually to the intraoperative situations.
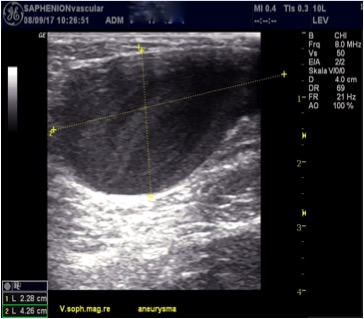
Sealing veins protocol: Aneurysma 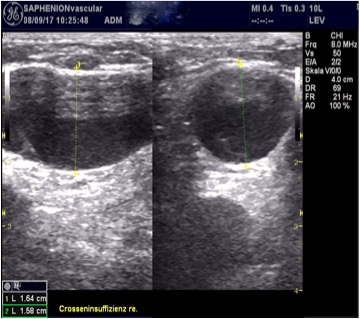

Sealing veins protocol: vein junction
Sealing vein protocol: VenaSeal of aneurysmatic junction left side in case of 57 years old women (left pictures), Sealing GSV junction (right picture)
Sealing vein protocol – effective modifications from our point of view:
1.The tip of the VenaSeal catheter is placed ultrasound – controlled between 1 – 2 cm at the junction with the respective deep vein (pelvic/ femoral vein, popliteal vein). There succeed then both an almost stump free occlusion of the trunk vein, at the same time also side veins are closed during sealing the GSV or SSV or accessory saphenous vein.
2. Injections are performed in a 3 – to – 4 rhythm, always 3 to 4 injections every 2 to 3 cm for about 9 to 12 cm and simultaneous sliding compression by 4 fingers of the hand. The compression with the hand and the fingers is compared to the compression with the transducer significantly better dosed and also allows a differentiated compression in lower – lying trunk veins (obesity). The fingers of the human hand can feel the catheter tip well and it succeeds in a much better dosage of venous compression – the adhesive polymerizes in contact with the vein wall.
3. At junctions of accessory saphenous veins or connecting veins in the course of the truncal vein, we inject an additional drop of the vein glue to close the junction of these vessels also over a length of 2-3 cm. For dilated veins and venous aneurysms, we set glue points every 1.5-2 cm. Thus, the closure of extended veins up to 3 cm in diameter is no longer a problem.
4. The injections are continued until the black mark of the Teflon catheter, with an existing lateral branch varicosis we also place a glue injection behind the marking. Thus, lateral or side branch veins can be closed in the junction area with the vein glue.
5. By intraoperative measurement of venous diameter as well as pressure and flow measurement via a catheter in the varicose vein (lying patient), additional information can be obtained on whether we put a glue drop every 1.5 cm or every 3 – 4 cm.
6. Another important point is the positioning of the patient on the operating table, Trendelenburg or Anti – Trendelenburg position. This depends on the one hand on the diameter, but also on intraoperatively measured venous pressure in the truncal vein. As a rule, by this rearrangement alone a good volume/pressure reduction in the truncal varicose vein can be achieved
7. Also, the application of the vein glue by Seldinger needles or cannulas works very well. This, however, is reserved for the side branch varicose veins and the perforator veins.
8. Of course, all of these modifications to the approved protocol should be discussed with the patient prior to the procedure and the cause and potential side effects should be identified. However, it would be desirable that the company Medtronic may cause additions to the protocol to f.e. to solve the problem of the long venous stump of the junction
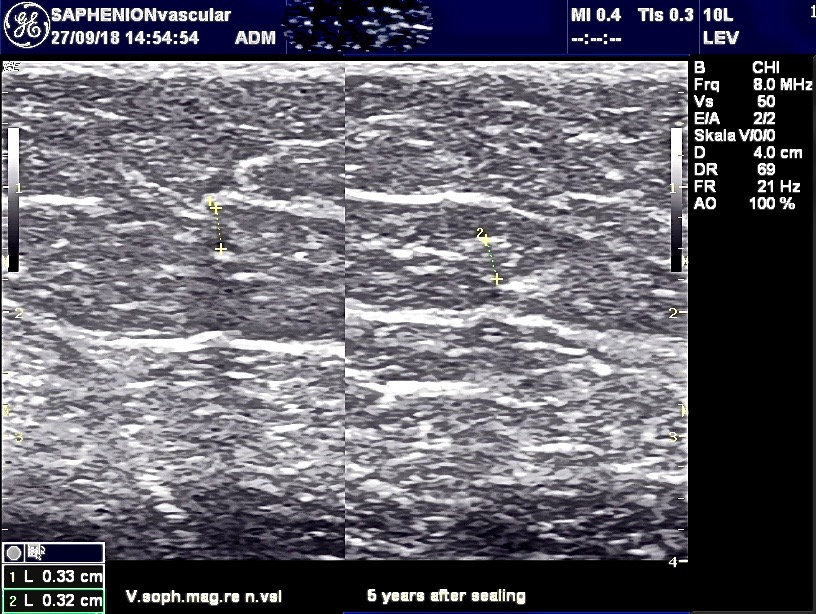
Sealing veins protocol – 5 years after therapy of GSV 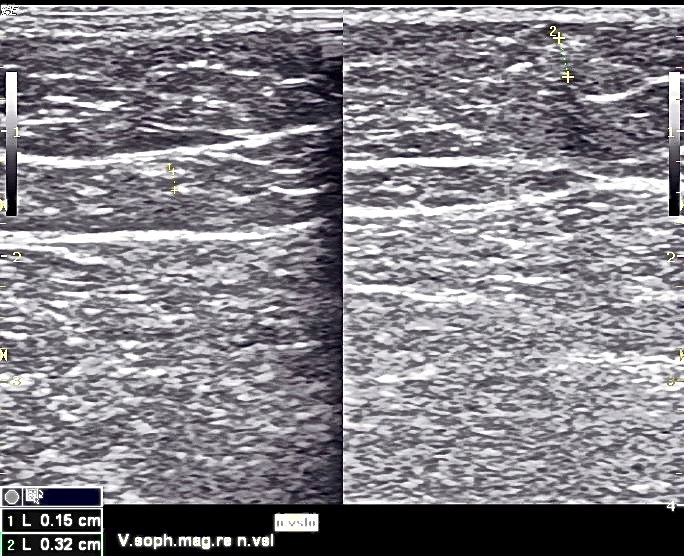
Sealing veins protocol – 5 years after therapy of GSV
Ultrasound examination 5 years after VenaSeal therapy simultaneously GSV both legs and SSV left leg in a 73 – years old patient: veins have completely disappeared, no glue residues presentable.
Links / Rerences:
Herberer G. und RJAM van Dongen: Gefäßchirurgie; Springer Verlag Berlin, Heidelberg, New York, Tokyo, London, Paris, 1982: S.722 – 739
Kremer K., Schumpelick V. und G.Hierholzer: Chirurgische Operationen – Atlas für die Praxis; G.Thieme Verlag, Stuttgart, New York,1992: S.682 – 685
Weber, J. und May, R.: Funktionelle Phlebologie; Georg Thieme Verlag Stuttgart, New York, 1990: S. 531 – 543
https://www.ncbi.nlm.nih.gov/pubmed/?term=recidive+after+endovenous+therapy
https://www.thieme-connect.de/products/ejournals/abstract/10.1055/a-0798-6120
https://www.ncbi.nlm.nih.gov/pubmed/28181899
https://www.journalijdr.com/sites/default/files/issue-pdf/15326.pdf
https://www.ncbi.nlm.nih.gov/pubmed/23032495
https://www.ncbi.nlm.nih.gov/pubmed/27898181
https://www.ncbi.nlm.nih.gov/pubmed/24176098
https://www.ncbi.nlm.nih.gov/pubmed/18431342
https://www.ncbi.nlm.nih.gov/pubmed/17598080
https://www.ncbi.nlm.nih.gov/pubmed/29914814
https://www.ncbi.nlm.nih.gov/pubmed/27126643
https://www.journalijdr.com/sites/default/files/issue-pdf/15326.pdf
http://vascular-endovascular-therapy.imedpub.com/sealing-veins-vs-radiofrequency-ablation-oftruncal-varicose-veins5-years-experience.pdf
Editors | Journal of Vascular and Endovascular Therapy |
| Editors | Journal of Vascular and Endovascular Therapy |Editorial Board of Journal of Vascular and Endovascular Therapy consists − eminent scientists, scholars, researc… |
Pictures:
Feliks Büttner, Bahnhofsgallerie Teterow
Ultrasound pictures: Saphenion Utzius